
Diaphragmatic hernia: symptoms and treatment
 Diaphragmatic hernia - displacement in the thoracic cavity of the abdominal organs, which occurs through the esophageal opening of the diaphragm( therefore the disease has another name - hernia of the esophageal opening of the diaphragm).It is a chronic disease with recurrent relapses, significantly impairing the quality of life.
Diaphragmatic hernia - displacement in the thoracic cavity of the abdominal organs, which occurs through the esophageal opening of the diaphragm( therefore the disease has another name - hernia of the esophageal opening of the diaphragm).It is a chronic disease with recurrent relapses, significantly impairing the quality of life.
Diaphragmatic hernia is a more common disease than it may seem.It occurs in 0.5% of the population, but half of the patients do not have a clinic, they do not go to the doctors, and the diaphragmatic hernia remains unidentified.
Contents:Causes of
Diaphragmatic hernia is formed due to the fact that the connective tissue membrane that is located between the esophagus and the aperture of the diaphragm is stretched, through which the esophagus passes from the thoracic cavity to the abdominal.
The reasons why the esophageal aperture of the diaphragm increases in size, are not fully understood. Factors contributing to membrane weakness and dilatation of the esophageal opening of the diaphragm:
- genetic insufficiency of the connective membrane tissue;
-
 increased intra-abdominal pressure;
increased intra-abdominal pressure; - predisposition to hiccups - convulsive contractions of the diaphragm;
- the patient's propensity to reflux - the reverse ingestion of food from the stomach into the esophagus ;
- age-related changes in the membrane between the esophagus and diaphragm, due to which it loses its elasticity;
- esophageal displacement upward.
In turn, esophageal displacement is observed with:
- dyskinesia of the digestive tract( abnormalities of natural muscle contractions);
- pathological conditions of the esophagus itself - scars, tumors, luminal narrowing.
The genetic factor is confirmed by the fact that the hernia of the esophageal opening of the diaphragm often occurs in people with other congenital disorders from the connective tissue - with :
- flat feet;
- Marfan syndrome( such patients are tall, with long limbs and elongated fingers).
 The most common factor contributing to the weakness of the membrane is the age-related changes in it. Young people may suffer from frequent respiratory and digestive diseases accompanied by coughing, reflux and vomiting, but with no diaphragmatic hernia.On the other hand, the cases of hernia of the esophageal opening of the diaphragm sharply increase after 60 years - even if such patients at a younger age did not suffer from ulcers or bronchitis, adhered to the correct diet and did not suffer from reflux, eructation, vomiting or hiccough.
The most common factor contributing to the weakness of the membrane is the age-related changes in it. Young people may suffer from frequent respiratory and digestive diseases accompanied by coughing, reflux and vomiting, but with no diaphragmatic hernia.On the other hand, the cases of hernia of the esophageal opening of the diaphragm sharply increase after 60 years - even if such patients at a younger age did not suffer from ulcers or bronchitis, adhered to the correct diet and did not suffer from reflux, eructation, vomiting or hiccough.
The immediate cause most often provoking the appearance of diaphragmatic hernia is an increase in intra-abdominal pressure. It is observed under such conditions and processes as:
- strong flatulence;
- frequent and protracted diseases of the respiratory system, accompanied by frequent bouts of coughing;
- chronic diseases of the gastrointestinal tract, accompanied by frequent vomiting;
- free fluid in the abdominal cavity( ascites);
- tumors of huge dimensions in the abdominal cavity;
- pregnancy.
The most common cause of increased intra-abdominal pressure is cough.
Development of the disease
Before passing into the stomach, the esophagus passes into the abdominal cavity through the esophagus of the diaphragm, with which it is connected along the circumference by a connective tissue membrane.Thanks to her, the tightness between the abdominal and thoracic cavities is ensured.This membrane is quite elastic - when pressure builds up in the abdominal cavity, it is capable of stretching.
Because of frequent contractions( or congenital insufficiency), the connective tissue elements of the diaphragm-esophageal membrane soon wear out and cease to act as a shock absorber - the tightness between the thoracic and abdominal cavities is disrupted.With subsequent increases in abdominal pressure, the organs of the abdominal cavity are pressed against the weakened membrane - after a while it is no longer able to hold the abdominal organs, which, as the intra-abdominal pressure rises, rushes into the thoracic cavity.So there is a hernia of the esophageal aperture of the diaphragm.
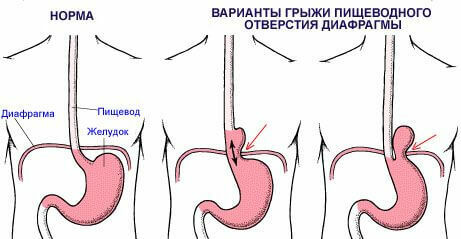
The most common types of hernia are:
- sliding - when the thoracic cavity leaves the area where the esophagus passes into the stomach, and the fragment of the stomach itself;
- paraesophageal - esophageal-gastric transition remains in the abdominal cavity, but part of the stomach penetrates through the esophagus and is located above the diaphragm.
Sliding hernia in most cases is determined by accident - it is found in 40% of patients who perform chest x-ray for some other reason.
Often the hernia of the esophagus is not observed as a separate disease, but is part of the so-called triad states, when the patient simultaneously has pathologies from different organs and systems. As an example - Castan's triad: in addition to a hernia of the esophageal opening of the diaphragm, chronic cholecystitis and ulcer of the duodenum are also observed.
Therefore, if a patient has a violation of the gallbladder, stomach or intestines, it will be superfluous for him to be examined for hernia of the esophageal opening of the diaphragm.
Symptoms of diaphragmatic hernia
The most frequent and typical symptoms by which a patient can suspect a hernia of the esophageal opening of the diaphragm are:
- pain;
- signs of reflux - the return of the contents of the stomach into the esophagus.
Pain occurs:
-
 when a part of the stomach penetrates the chest cavity, its nerve endings are squeezed;
when a part of the stomach penetrates the chest cavity, its nerve endings are squeezed; - with reflux accompanying diaphragmatic hernia, the acid content of the stomach enters the esophagus and irritates its mucosa;
- because of constant reflux, the walls of the esophagus stretch, thus irritating their nerve endings;
- Less commonly, pain occurs due to spasm of the esophagus and a fragment of the stomach that has entered the thoracic cavity through the esophagus of the diaphragm.
Pain characteristics with diaphragmatic hernia:
- sensation - dull;
- is moderate in intensity, patients are able to sustain it;Severe pain is extremely rare;
- is located most often in the upper third of the sternum;
- can spread along the esophagus;
- in some cases gives in the back and between the shoulder blades;
- grows when you try to bend.
- In most cases, the pain appears:
- after eating( especially abundant);
- during or after exercise;
- during cough;
- with bloating;
- in prone position.
Characteristic is that such pain disappears after:
- eructations;
- vomiting( sometimes patients with the goal of relief cause it artificially);
- deep inspiration;
- transition to vertical position;
- water intake or alkaline solutions.
-
 burping - venting of gases from the stomach through the mouth, often with food particles;
burping - venting of gases from the stomach through the mouth, often with food particles; - regurgitation - throwing a small portion of food from the stomach into the esophagus, and from there into the mouth;In fact it is vomiting in its minimal manifestation;
- obstruction of food passage through the esophagus;
- pain at the time of ingestion;
- heartburn;
- hiccup;
- burning sensation and pain in the tongue.
- observed almost immediately after eating;
- is very pronounced, sonorous;
- during an eructation in the mouth is felt sour taste( due to acidic gastric contents), often with a bitter aftertaste( due to the impurity of bile).
- is most often observed after eating( especially when lying down);
- in half the cases can bother at night( the so-called "wet night pillow" symptom);
- observed regurgitation of food, and if repeatedly, after a short time - with acidic stomach contents;
- most often regurgitates a small amount of stomach contents - from 10 to 20 ml, but with an exacerbation of signs of diaphragmatic hernia, the volume of regurgitated food can be 2-3 times larger.
- the patient complains of an uncomfortable pressing feeling behind the sternum during the act of swallowing - often characterizes him "Like a stake";
- such difficulty in the passage of food through the esophagus is caused by taking too hot or too cold a liquid, eating food in a hurry or in a stressful situation;
- a physiological paradox is observed: with dysphagia, solid food passes through the esophagus, albeit with difficulty, but much easier and faster than liquid or semiliquid.
- is noted immediately after eating;
- is more pronounced if the patient has taken a recumbent position;
- very often occurs at night, even if after eating a few hours have passed;
- is often unbearable by subjective perception, the patients say that it is easier for them to tolerate pain with a hernia than with heartburn.
- is provoked by ingestion;
- manifests itself in the form of protracted seizures lasting several hours, and in severe cases - and several days.
- infringement;
-
 solarium;
solarium; - gastrointestinal bleeding;
- ulcer of the esophagus;
- narrowing and / or shortening of the esophagus;
- perforation of the esophagus( formation of a through hole in the wall of this organ);
- displacement of the gastric mucosa in the esophagus;
- chronic inflammation( gastritis), and then ulcer of that part of the stomach, which because of the displacement often occurs in the chest cavity;
- reflex disorders in the work of the heart - the so-called reflex angina;
- anemia.
- pain enhancement;
- nausea and multiple vomiting with an admixture of blood;
- disorders of the cardiovascular system - pronounced dyspnea, accelerated heartbeat, sharply lowered arterial pressure, blue skin of the patient;
- , the lower part of the thorax seems to bulge, lagging behind in the breath;
- on the roentgenogram, chest organs are biased in a healthy way.
- painful sensations sharply increase, become intense;
- basically pains bother in the upper abdominal floor, but can be felt in the left hypochondrium, as well as in the area between the shoulder blades;
- on the nature of pain at first resemble fights, then become permanent;
- pain syndrome is not removed by ingestion of food, water or staying in any position;In rare cases, the pain subsides slightly in the patient's position on the left side.
- pains become more intense, burning;
- pains are amplified by pressing on the area of the solar plexus;
- pain relief occurs if the patient takes a knee-elbow position or leans forward.
- the stomach or bowel loop very often migrate from the abdominal cavity to the thoracic and back;
- this provokes a traumatism of the vessels passing in the mucosa and under it;
- after a while, the traumatization results in a violation of the integrity of the walls of the vessels, bleeding begins.
- vomiting of blood appears in the vomit;
- stool - dark, semi-liquid;
- deterioration of the general condition of the patient - weakness, apathy, lethargy;Deterioration of red blood indices.
- .
- general weakness;
- frequent dizziness;
- darkening and "flies" before the eyes;
- pallor of the skin and visible mucous membranes.
- dry skin;
- brittleness and blotchiness of nails due to disruption of their nutrition;
- a perversion of taste and smell.
- of red blood cells;
- hemoglobin.
- radiography withContrast;
- fibroscopy;
- Ezofagomanometry.
- inflammation, erosion, bleeding, ulcers of the esophagus and stomach;
- A shortening of the esophagus, which is determined by detecting a decrease in the distance from the patient's canines to the stomach( measured by the probe itself).
Symptoms reflux :
Belching - is the most common symptom of reflux.Its characteristics with diaphragmatic hernia are as follows:
Regurgitation of with diaphragmatic hernia has such characteristics :
Dysphagia develops as a result of impaired passableness in the esophagus, but this is not a permanent sign of diaphragmatic hernia.Characteristics of dysphagia:
Pain sensations behind the breastbone appear only in the presence of reflux.
Heartburn - is one of the most revealing signs of the diaphragmatic hernia .In some patients, it is the leading sign of diaphragmatic hernia. Heartburn features for hernia of the diaphragm:
Hiccup is observed in a small number of patients with diaphragmatic hernia( according to different data - from 3 to 7%). But in the absence or paucity of other symptoms, it may lead to the idea of a hernia.Hiccups are explained by the fact that the hernial protrusion irritates the diaphragmatic nerve, which causes chaotic rampant contractions of the diaphragm. Characteristics of hiccups with diaphragmatic hernia:
Burning and pain in the language are manifested when the reflux is expressed - throwing acidic stomach contents into the oral cavity, which causes a burn of the mucous membrane of the tongue.This content can also enter the larynx, causing hoarseness.
In most cases, the diaphragmatic hernia is asymptomatic.First of all, this concerns the options, when only the fragment of the stomach penetrates into the thoracic cavity( para-esophageal hernia).Sliding hernias are clinically more indicative and in some cases are manifested by pain and signs of reflux.
At the same time, complications are more characteristic of paraezofagal hernias.
Complications of diaphragmatic hernia
In addition to the fact that diaphragmatic hernia can be detected accidentally, it is often diagnosed because of the complications of .There are many complications of hernia of the esophageal aperture of the diaphragm. Highlights this:
Infringement is the most complex and dangerous complication of hernia of the esophageal opening of the diaphragm. It occurs when the organ of the abdominal cavity, hitting the esophageal aperture of the diaphragm, can not slip back and is squeezed in the hernial sac, and also around the circumference of the sac due to the contraction of the connective tissue elements of the membrane between the opening and the esophagus. Signs of infringement:
The most indicative sign of infringement of a diaphragmatic hernia is pain. Their characteristics are as follows:
Solar - is the damage to the solar plexus .The plexus itself is a tangle of vegetative nerve fibers, which are affected in many cases again, due to some other diseases - in this case because of the diaphragmatic hernia. Signs that the diaphragmatic hernia has become more complicated with solarate:
Bleeding sooner or later complicates the diaphragmatic hernia .Acute severe bleeding affects about 20% of patients, hidden - about 25%.The most common cause of bleeding in the hernia of the esophageal opening of the diaphragm are ulcers and erosion of the esophagus and stomach. The mechanism of such bleeding is as follows:
Often, bleeding complicating the diaphragmatic hernia is provoked by vomiting.
Signs of gastrointestinal bleeding with diaphragmatic hernia:
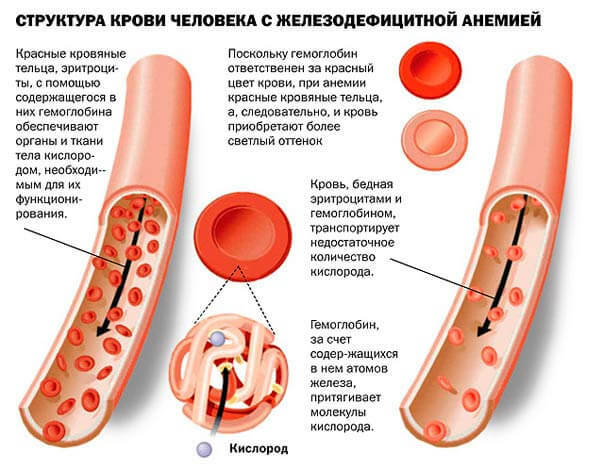
With hernia of the esophageal opening of the diaphragm, anemia most often develops not because of acute massive bleeding, but because of the permanent latent .This is iron deficiency anemia.
Less often, anemia occurs due to the fact that due to permanent displacements in the chest cavity, the upper part of the stomach at which vitamin B12 is produced is atrophied.
The sudden appearance of anemia in a previously unaffected person needs to be paid close attention, since it can be the only sign of a hernia of the esophagus of the diaphragm ( recall that such hernias are often asymptomatic).In fact, it is not sudden, its development is preceded by repeated hidden bleeding.Hidden - means that there are no visible discharges of blood from the gastrointestinal tract, the blood can only change the feces( it becomes semi-liquid and dark as tar - that's why it appears officially as "tar-like feces").
Manifestations of anemia complicating diaphragmatic hernia are quite typical for anemia in general:
But the fact that this anemia is iron deficient and indicates diaphragmatic hernia in the absence of its other symptoms is evidenced by the so-called sideropenia syndrome, which includes:
Anemia is confirmed by a worsening of the blood test - low in :
Diagnosis
Since the hernia of the esophageal opening of the diaphragm is asymptomatic( at least uncomplicated), is of great importance in the early diagnosis of this disease, there are additional survey methods - primarily instrumental :
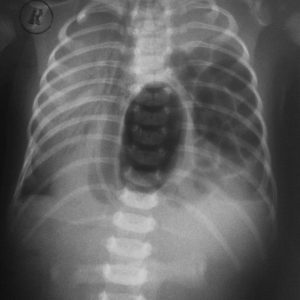 Radiography using contrast medium is the most significant method in the diagnosis of diaphragmatic hernia.
Radiography using contrast medium is the most significant method in the diagnosis of diaphragmatic hernia.
The patient is given a drink of a suspension of barium sulfate, which fills the stomach, esophagus and allows to determine their contours on the roentgenogram.In particular, you will see the part of the stomach that has fallen out in the chest cavity, the shape, size and bends of the esophagus, as well as the location of the esophageal aperture of the diaphragm, which on the X-ray photograph appears as a "notch" on the contours of the stomach.
Radiography with contrast allows also to reveal and clarify details when pinching the diaphragmatic hernia - it is determined by the characteristic "bubble" with air.
Fibroscopy - examination with the probe equipped with special optics that helps to see the gastrointestinal tract from the inside and to detect its changes due to the diaphragmatic hernia:
Due to the formation of the diaphragmatic hernia above the diaphragm, a zone of increased pressure is determined, which is measured during esophagomanometry.Decoding the measurement data will help determine the state of the esophageal aperture of the diaphragm.
Laboratory methods of examination of special significance in diagnosis of hernia of the esophageal opening of the diaphragm do not have . A blood test will help identify anemia and, in the absence of any symptoms, suspect a latent bleeding that may indicate a diaphragmatic hernia.
Treatment of diaphragmatic hernia
 If a small piece of stomach enters the chest cavity without clinical consequences for the patient, no specific treatment is performed. It is enough to adjust the diet and exercise so that the patient can avoid discomfort, if any, in the absence of them - to prevent the occurrence of such feelings.
If a small piece of stomach enters the chest cavity without clinical consequences for the patient, no specific treatment is performed. It is enough to adjust the diet and exercise so that the patient can avoid discomfort, if any, in the absence of them - to prevent the occurrence of such feelings.
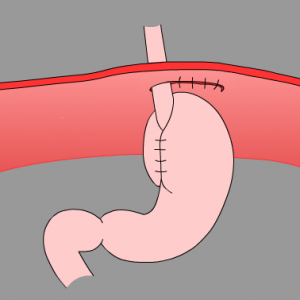
If a disease progression is observed during repeated instrumental examination( an increase in the diameter of the diaphragm's esophageal opening, an increase in the abdominal abdominal cavity's residence time, the occurrence of complaints), such a hernia should be operated to avoid the risk of infringement. The aim of the operation is to narrow the enlarged esophageal aperture of the diaphragm and to strengthen it.
When the diaphragmatic hernia is restrained, if the signs do not decrease or even build up, surgical intervention is carried out urgently.
Prevention
To prevent the occurrence of a diaphragmatic hernia, the causes of its occurrence and the provoking factors should be eliminated, primarily diseases of the respiratory system with frequent coughing, gastrointestinal diseases with vomiting, flatulence, loose fluid in the abdominal cavity.Often, the diaphragmatic hernia regresses after childbirth.
Forecast
With the right medical approach, the forecast is favorable .Infringements of diaphragmatic hernia with all the ensuing consequences( in particular, necrosis of impaired content) occur much less frequently than infringements with other hernias.
Kovtonyuk Oksana Vladimirovna, medical reviewer, surgeon, medical consultant


