Myomatous node
 The myomatous node is a formation in the uterine wall of benign origin formed from smooth muscle and connective structures. Contrary to the very popular belief, the myomatous node has only some signs of a true tumor, but in fact it is not. It is more appropriate to correlate it with a tumor-like formation. So, for example, from a true tumor, the myomatous node is distinguished by its close connection with the level of hormones( especially estrogens), as well as the unique ability to regress independently.
The myomatous node is a formation in the uterine wall of benign origin formed from smooth muscle and connective structures. Contrary to the very popular belief, the myomatous node has only some signs of a true tumor, but in fact it is not. It is more appropriate to correlate it with a tumor-like formation. So, for example, from a true tumor, the myomatous node is distinguished by its close connection with the level of hormones( especially estrogens), as well as the unique ability to regress independently.
Since the myomatous nodes are associated with the level of estrogens, they are more often diagnosed during the period of the greatest hormonal activity of the ovaries. The "favorite" age of myomatous nodes is the period from 20 to 40 years, among other age groups they are less common.
The advent of modern, high-precision diagnostic equipment has turned myomatous nodes into a common disease( 30% of patients with gynecological pathology).However, the presence of a myoma node does not always imply the need for serious treatment. There is an opinion that the myomatous nodes can form and independently regress in many, including gynecologically-sound, women. This assumption is based on the frequent diagnosis of asymptomatic small-sized myomatous nodes, which after a short period of time in the uterus are no longer detected.
At the research stage there are reasons for the formation of myomatous nodes in the uterine wall. One of the causes of myomatous node development is considered to be hormonal dysfunction. The increase in the amount of estrogen provokes the growth of the nodes, and the estrogen deficiency in menopause leads to a decrease. Against the background of postmenopause, when the hormonal function of the ovaries completely faded, the myomatous nodes often disappear permanently.
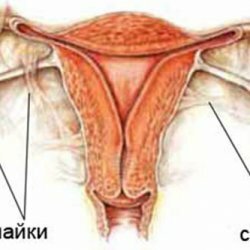
To understand the mechanism of formation and growth of the myomatous node, it is necessary to imagine how the uterine wall is arranged. It forms three layers:
- Outer( perimeter) serous layer. It covers the uterus from the outside, in structure it is similar to the peritoneum;
- Internal( endometrium) mucous layer. Lining the cavity of the uterus from the inside, represented by layerwise arranged rows of flat epithelium. The functional layer( the one located on the surface of the uterine cavity) of the endometrium is closely related to cyclic hormonal changes and monthly undergoes rejection and recovery processes.
- Medium( myometrium) muscle layer. The thickest and most powerful layer of the uterine wall. In fact, it is a large muscle with a very complex structure.
Myometrium serves as the birthplace of the myomatous node. The size of the myomatous node does not always correspond to the clinical picture, but it is always taken into account when deciding on the question of surgical treatment.
There are often several nodes in the uterus, each of which can differ both in the stage of development and in the type of growth. The growth of myoma nodes serves as an important diagnostic criterion.
For selection of medical tactics, it is important not only the growth rate of the node, but also its localization. The node formed in the myometrium may remain in the myometrium, and may begin to grow toward the adjacent layers of the uterine wall.
With myomatous nodes, menstrual irregularities, pains of various character, infertility can be observed. Often, clinical manifestations are absent. Symptoms of the myomatous node are not specific, so an accurate diagnosis can be made only after additional instrumental research( ultrasound, gyroscopy).
Treatment of myoma nodes has a large number of options and varies from simple dynamic observation to surgical intervention.
Allied myomatous node
All myomatous nodes are initially formed in the muscular layer, therefore, modified smooth muscle cells and connective tissue predominate in their structure. Growing and thickening, the knot can begin to "move" towards the uterine cavity. As a result, the localization of the myomatous node changes. When the myomatous node is located in the submucosal layer, it is called submucous.
The submucosal localization of the myomatous node refers to the most unfavorable clinical situation. Regardless of the size and growth rate, submucous nodes already in the early stages of development provoke a vivid clinical picture and cause serious complications.
Submucous myomatous node protrudes into the uterine cavity and deforms it. Menstruation becomes painful and plentiful. Over time, when the knot becomes large, menstruation loses its cyclicity.
Prolonged and profuse menstrual bleeding is also provoked by a violation of the tonus of the muscular wall due to the presence of a myomatous node in it.
The submucous myomatous node present in the uterus remains asymptomatic for a very short time, then it is perceived by the uterus as a foreign body. Reflexively, the uterus tries to free itself from it with the help of strengthened contractions. As a result, there are strong cramping pains similar to labor pains, and the knot, like a fetus, is pushed outward, accompanied by heavy bleeding. Figuratively, this situation is described as the "birth" of the myoma node. The patient's condition requires immediate hospitalization and surgical treatment.
Serious consequences of the submucosal myomatous node can be avoided if in time to diagnose its presence in the uterus. As a rule, the primary diagnosis of submucosal nodes begins with a patient's questioning and palpation of the pelvic area. The increase in the size of the uterus, the unevenness of its contours and the change in density indicate a potential presence of myomatous nodes. However, palpation features are always indirect, and they can not determine the precise localization of nodes. Reliable information is provided by ultrasound, which determines the deformation of the uterine cavity and the presence of a nodular formation in it.
Subserous myomatous node
The subserous( subperitoneal) arrangement of the myomatous node is said to start growing in the opposite direction from the uterine cavity. More than half of all the occurring myomatous nodes( 55%) have a subserous location.
The formation of the node begins at the border of the myometrium and the outer, serous, envelope of the uterus, and then, as it grows, the knot rushes toward the abdominal cavity.
A distinctive feature of subserous myomatous nodes is their weak connection with the muscular wall of the uterus. Often the intensive growth of nodes occurs already in the subperitoneal, and with the myometrium they are connected only by a thin, long base - the leg, which contributes to the large mobility of the node. In case of torsion of the leg of the myomatous node, a clinic of the "acute abdomen" arises, associated with painful pains and a sharp deterioration in the state of health. If the food is damaged in the leg zone, necrosis of the myomatous node develops. Necrosis leads to suppuration and destruction of tissues in the site of the node, there are not only sharp pains, but signs of infectious inflammation. Necrosis of the myomatous node of any localization( including subperitoneal) leads to purulent fusion of uterine structures and the formation of the uterine cyst.
A large-sized subserous myomatous node reaches infrequently, in half of patients it remains very small for a very long period of time, not manifesting itself clinically, and is diagnosed accidentally. In the other half of the patients, the subperitoneal nodes, expanding, overstretch the serous cover that covers them, thereby provoking constant aching pelvic pains that increase during menstruation.
Menstrual function with subserous arrangement of myomatous nodes is disrupted only if they are of considerable size. As a rule, there are abundant menstruation.
Located outside the uterus, the subserous myomatous node, in case of its considerable size, can interfere with the work of neighboring organs: the bladder in front and the rectum behind the uterus.
Diagnosis of the subserous myoma node begins with palpation of the pelvic region. An increase in the density of the uterus, deformation of its outer contour, can be detected. If the node has a leg, it can be displaced by probing. Small myomatous nodes on a broad base, as a rule, are not palpable, but their presence is indicated by the asymmetry of the uterine contours.
More precise information about the myomatous node of the subserous localization is provided by ultrasound scanning. On the screen, a well-displaceable, rounded formation with a common unbroken contour( that is, tightly welded to it) is well visualized, with a thin stem - without the effect of "ingrowing" into the muscular wall.
For more reliable information about the condition of the uterine surface and surrounding structures, laparoscopy can be performed. The method allows you to directly examine the uterus from the outside and perform differential diagnosis of the subperitoneal myoma node and ovarian tumor.
Interstitial myomatous node
When the developing myomatous node grows only within the muscular wall of the uterus, it is called interstitial. Uncommon situations occur when the initial interstitial myomatous node, reaching a significant size, is able to leave the myometrium.
Interstitial myomatous node often grows long and does not manifest clinically. It can be diagnosed accidentally. The intramuscular nodes have no legs and are practically not subject to destruction due to a malnutrition, therefore complications in the form of torsion of the base and / or necrosis are uncharacteristic of them.
Located in the muscular wall of the uterus, the interstitial myomatous node deforms its contractile function. As a rule, the uterine wall loses its former tone, and the muscle contractions do not occur synchronously. Therefore, menstruation with a saved rhythm becomes more abundant and more prolonged.
Large blood loss during menstruation can trigger the symptoms of anemia. There is weakness, dizziness, a woman quickly gets tired.
As a rule, the size of the myomatous node affects the character of the menstrual function: the more it is, the more pronounced the menstrual changes. Also, the painful syndrome depends on the size of the knot: if the knot is large, aching, not pronounced pains appear.
The number of myomatous nodes is not inferior in importance to their magnitude. Multiple nodes of even small size can stretch the cavity and increase the surface area of the uterus, and this also provokes greater menstrual blood loss.
Large single or small multiple myomatous nodes increase the size of the uterus and its weight, thereby increasing the load on the ligamentous apparatus. The ligament supporting the uterus is stretched by the "weighted" uterus, there are constant pains of different intensity.
Unfortunately, if the interstitial myomatous node "grows up" slowly, the first soft symptoms are ignored. Changes in menstrual function and mild pains of the patient correlate with harmless causes and eliminate them( often successfully) on their own.
Intramural myomatous node
The term "intramural", like most medical definitions, comes from the Latin word form intra( inside) + murus( wall), meaning the localization of something in the wall of a hollow organ.
Intramural myomatous nodes are diagnosed more often than sites of other localization. They can be single or multiple, small or large in size, and also be combined with myomatous nodes of other localization.
The terms "intramural" and "interstitial" are essentially identical and refer to the same for myomatous nodes - their localization within the muscular layer of the uterine wall.
Thus, everything said about the interstitial myomatous nodes, applied to the intramural nodes.
The problem of the influence of myoma nodes on reproductive function is also related to their effect on the ability to conceive or tolerate a child. Moreover, more important is not the presence of the myomatous node, but its magnitude and location.
If the nodes are localized in the corners of the uterus, they can become a mechanical obstacle to the movement of the fertilized egg into the uterine cavity, and the node located in the region of the posterior uterine wall hinders its proper implantation. When the egg is fixed lower, closer to the cervix, the pregnancy is interrupted much earlier than the due date.
If there are small multiple myomatous nodes in the uterus, they often do not complicate pregnancy and childbirth. But a large single myomatous node during pregnancy can provoke many negative consequences: miscarriage or early birth, bleeding during or after childbirth, untimely detachment of the placenta.
Intramural myomatous node during pregnancy behaves ambiguously. With the onset of pregnancy, the ratio of sex hormones changes, and in the tissues of the uterine wall, structural changes begin. In the first eight weeks of pregnancy, the myomatous node may increase, and then stop growing or even significantly decrease in size.
The disappearance of myomatous nodes during pregnancy is possible if the basis of development is an excess of estrogens, during pregnancy against a background of hypoestrogenesis, the nodes begin to decrease.
Sometimes the disappearance of myomatous nodes in pregnant women is not due to their reverse development, but to the expansion of the uterine wall, when the nodes are stretched together with the myometrium and are not visible during ultrasound scanning. As a rule, when you re-scan the uterus after childbirth, you can find them again.
Treatment and removal of the myomatous node
The magnitude, location and growth of myomatous nodes are taken into account when choosing therapeutic tactics.
Contrary to the misconception of many patients, the myomatous nodes are not always operated. Also they are not always subjected to any other therapy. Small asymptomatic nodes without signs of rapid growth are sometimes observed for many years, and by the time of the completion of hormonal function of the ovaries in elderly patients, they independently decrease and disappear.
Conservative methods of therapy take into account the origin of the myomatous node. Drug treatment is advisable for uncomplicated nodes not exceeding 3 cm. If the patient refuses surgery, nodes can be treated and a little larger.
The most popular method remains hormone therapy. The treatment regimen and the list of medicines are always individual, as the hormonal background, the state of the immune and endocrine systems, the presence of complications are taken into account. Hormonal drugs are selected in such a way that they can simulate a normal menstrual cycle. For this purpose, gestagens( Duphaston, Progesterone, Utrozestan and the like) are used, combined estrogen-progestational agents( Janine, Yarina and the like).After 45 years, when the menstruation function is unreasonable, androgens are used.
The timing of treatment depends on the specific situation, but the presence of a positive effect in six months is necessary. If it does not, consider another treatment option - surgical.
So when is surgical treatment of myomatous nodes required?
1. With submucous site of nodes.
2. When the sizes of a uterus exceed those at 13-week pregnancy.
3. There is no effect of previous hormone therapy.
4. The nodes grow too fast( the uterus increases in a year more than four weeks of "pregnancy").
5. There are large subserous nodes( one or more).
6. The myoma node has a long leg.
7. In the nodes there are signs of torsion of the leg and / or necrosis.
8. If site localization provokes infertility.
In any operative treatment, the surgeon tends to keep the uterus and remove only the knot, but in the climacteric period the uterus is removed along with the nodes.
After the operation, the treatment does not end. If the cause of the development of the nodes in the uterus is not eliminated, they will appear again.