Painless myocardial ischemia

Many people believe that this diagnosis is a separate disease that is characterized by its own symptoms, but painless myocardial ischemia( hereinafter BIM) is an inseparable component of all existing ischemic diseases. According to European research centers, cases of acute ischemia occur in almost 50% of all patients for ischemic heart disease and 80% of these cases are not accompanied by any symptoms, in other words - painless.
What is BIM?
It should be noted that the definition of BIM is a documented indication of the process of transferring IHD disease without pain, without any discomfort in the thoracic part or in the chest. This disease has nothing like the symptoms that accompany the course of angina pectoris. A typical angina is another type of disease and should not be equated with BIM, since typical angina is characterized by localized pains or discontinuous, tolerable pain in the chest.
Epidemiology of BIM
The disease is very common and only according to previous data in the United States myocardial ischemia affects more than 3 million people, which is almost 5% of the total population and it's only those who suffer from BIM, and the number of people who have a different formIHD, is even greater. Today in the CIS countries the number of patients with ischemic heart disease and BIM is unknown, but with certainty it can be stated that in the percentage of patients we have more than in the US.
Classification of BIM does not yet exist, but there are several categories of it that are followed in the USA and Europe:
- Ischemia( painless) in persons with obstructed ischemic heart disease. These are patients who are completely free of symptoms and attacks of angina.
- A more common type of BIM, which includes patients who have had previous myocardial infarction.
- And the most common type of BIM: a disease in people with unstable, stable and variable angina.
In patients with CHD very often there is a variety of BIM, even more often than usual angina. There are many cases where the development of BIM with high physical effort has developed into a myocardial infarction with a subsequent fatal outcome.
In persons with BIM, such a risk exists to a much greater extent than in patients who have symptoms of ischemia.
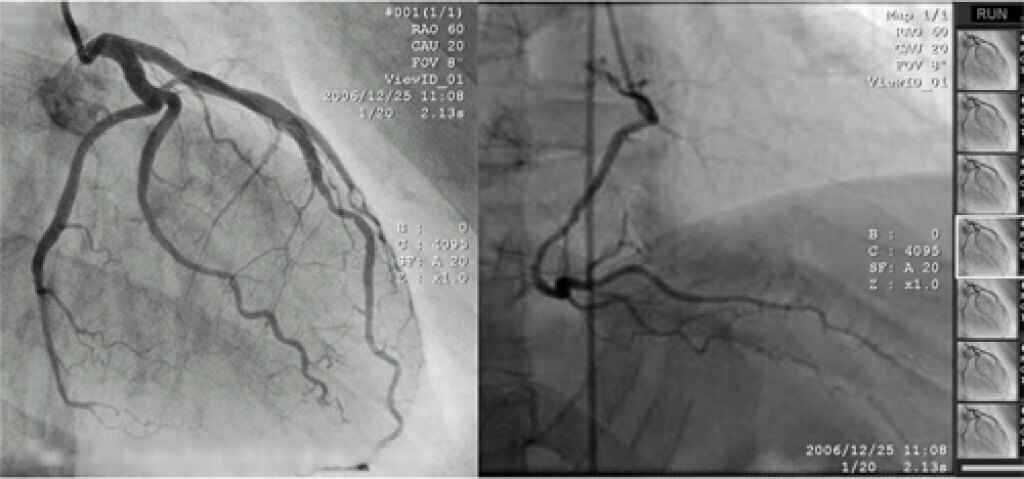
Ischemic heart disease has a variety of different symptoms, in the event of which it is necessary to immediately go through a complete examination for the detection of BIM.The simplest and most common method to determine the presence of BIM is a technique with physical exercise and ECG.But even such tests do not provide a 100% guarantee that the patient does not have BIM and all these results must necessarily be confirmed by echocardiography. To date, there is still no variety of tests and practical evidence that could confidently put the exercise method at the forefront of detection and prevention of BIM, as there are many subjective factors that can affect the quality of the test( blood pressure, diabetes mellitusetc.).But still, if a person is healthy and a complete blood test is performed before the BIM test, then the probability of determining an accurate diagnosis is 99%.
When examining healthy individuals, the choice is made in favor of a treadmill or veloergonometer, with which you can provide the patient with a relatively high burden on the body, in which the body will consume more oxygen, stimulating the heart for quick work. But no matter how the studies went and what they did not show, one thing remains unknown - why the patient does not show any pain and why there are no symptoms of the disease. Although it should be mentioned that painless ischemia often precedes myocardial infarction and the occurrence of anginal pains with shortness of breath.
What to treat: painless ischemia or angina?
There are also grounds to think that BIM influences well the functional state of the body as a whole and the left ventricle in particular. Is it possible to cure ischemia of the heart? On account of this, there are now great debates of many scientists who put forward their ideas and fought for establishing their personal theory. Some studies have shown that there have been significant improvements after the constant and systematic administration of antianginal drugs, which are always attributed to patients, but the fact is that mortality was increased precisely in those whose results were improving. There is also a theory that BIM can be very useful for the body, since it is the primary cause of the appearance of collaterals in the myocardium, which indicates that patients with BIM can experience more intensive development. Another group of scientists claims that it is necessary to fight with BIM and eliminate it in any measure, since repeated BIM can lead already to the destruction of the heart tissue. Myocardial ischemia can increase the degree of fibrosis and develop cardiac arrhythmia, promote the development of hypertrophy.
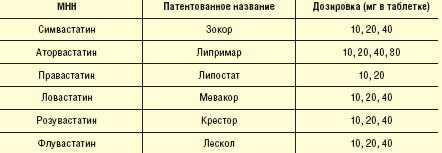
Many studies prove that it is possible to eliminate BIM as successfully as angina pectoris. This means that nitrates, adenoblockers and antagonists can also be used effectively in BIM, as well as in manifestations of angina pectoris. Moreover, studies prove that metoprolol proved to be much better for the treatment of BIM, rather than diltiazem. This drug significantly reduces the frequency and duration of attacks of ischemia of any type. But in the treatment of BIM, the very purpose of treatment remains unclear. What is better to concentrate on, to cure painless ischemia or to focus on angina? And as studies and practice show, it does not matter.
In any case, the unambiguous benefits of drugs for the treatment of BIM and the elimination of IHD symptoms have not yet been fully proven, so we should only hope for future studies in this field that were funded for 2012.