
Adrenal insufficiency

Adrenal insufficiency is a pathology that occurs against the background of insufficient hormonal secretion of the adrenal cortex, but may also be a consequence of problems with the hypothalamic-pituitary system. This disease provokes a water-electrolyte metabolism disorder, which can result in an adrenal crisis.
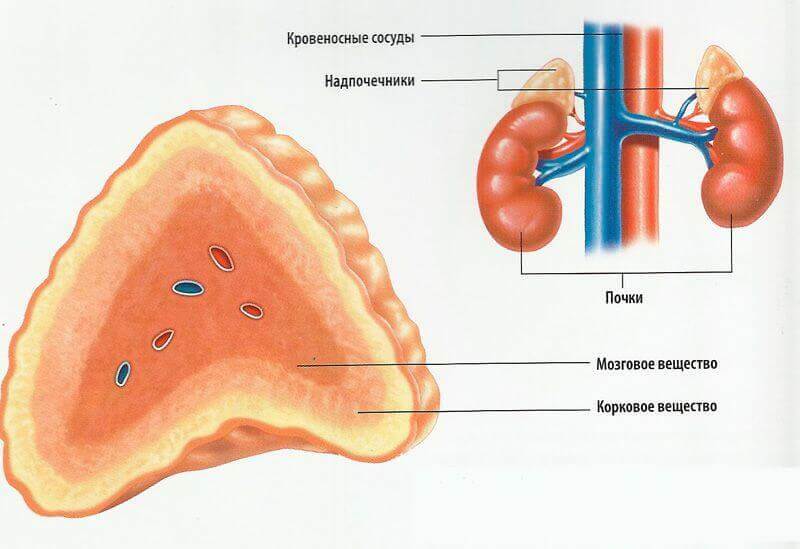
The cortex of the adrenal glands produces glucocorticosteroid and mineralocorticoid hormones.They are responsible for the main metabolic processes in the body tissues - protein, water-salt and carbohydrate, as well as for adaptation processes.Regulation of the adrenal cortex secretory level is the prerogative of the hypophysis and hypothalamus.
Table of contents: Classification of adrenal insufficiency Causes of adrenal insufficiency Adrenal insufficiency Symptoms Possible complications of adrenal insufficiency Diagnosis of adrenal insufficiency Adrenal insufficiency treatment Adrenal insufficiency prognosisClassification of adrenal insufficiency
This disease can occur in acute and chronic form.The acute form of adrenal insufficiency always proceeds in severe form, the patient's condition is greatly altered - the patient has an addisonic crisis, which is a decompensation of the chronic form of the disease.The chronic form of the pathology under consideration can be compensated, subcompensated and decompensated.

There is a differentiation of the disease under consideration to the primary and central form :
- Primary adrenocortical maldevelopment develops as a result of direct adrenal damage.It is this form of the disease being examined that is diagnosed in 90% of cases, most often in mature and old age.
- Secondary and tertiary( central) adrenal insufficiency is diagnosed rather rarely and is caused by disruption of the pituitary gland, which leads to atrophic changes in the adrenal cortex.
Causes of adrenal insufficiency
Most often( 98%), the cause of primary adrenal insufficiency is atrophic changes in the adrenal cortex of idiopathic .It is known that in this case autoimmune antibodies to the enzyme 21-hydroxylase are formed in the body, which destructively affect healthy tissues and adrenal cells.
The causes of the considered disease can be:
- Tuberculosis of the lungs.In this case, the doctors will diagnose the tuberculous defeat of the adrenal glands, which causes the development of the disease in question.
- Adrenoleukodystrophy is a rare genetic disease.In this case, a genetic defect of the X chromosome occurs and there is a lack of enzyme, which must break down the fatty acids.It turns out that the dystrophy of the adrenal cortex is provoked by fatty acids, which with this genetic defect accumulate in the tissues.
- Coagulopathies, bilateral adrenal infarction, metastasis of malignant tumors that have localization in the mammary gland or lungs, HIV-associated infections, surgical removal of the adrenal glands - these conditions are provoking factors regarding the primary form of the pathology in question.
- Severe suppurative diseases, syphilis, fungal infections and amyloidosis of the adrenal glands, malignant tumors, heart diseases, the use of certain medications( anticoagulants, steroidogenesis blockers, ketoconazole, chloridan, spironolactone, barbiturates) are predisposing factors that cause the development of adrenal cortex atrophy.
Secondary adrenal insufficiency can be triggered by abnormal processes in the hypothalamus or pituitary gland( tumor or structural disorder), resulting in a disruption of the corticotropic function, resulting in:
- of hypothalamus and pituitary gland neoplasms;
- diseases of the vascular system - for example, hemorrhages in the pituitary / hypothalamus, carotid aneurysm;
- pathological processes of granulomatous nature in the hypothalamus or pituitary gland;
- destructive and traumatic interventions: radiation therapy, conducted directly into the location area of the hypothalamus and pituitary, various surgical procedures, surgery, treatment with glucocorticoids for a long time.
characteristic will decrease the secretion of adrenal cortex hormones( cortisol and aldoaterona), the result becomes metabolic disorders and water-salt balance to primary adrenal insufficiency. If there is a deficiency of aldosterone, then there will certainly be progressive dehydration, which is caused by loss of sodium and potassium retention( hyperkalemia) in the body.In parallel, the patient will have functional disorders in the digestive system, heart and blood vessels - a provoking factor in this case is a violation of the water-salt balance.
During the progression of this pathology cortisol sharply decreases, resulting in degradation of glycogen synthesis processes and ultimately resulting in hypoglycemia .In conditions of cortisol deficiency, the pituitary begins to actively produce enzymes and melanocyte-stimulating hormone, which is manifested by active pigmentation of the skin and mucous membranes.Numerous physiological stresses( such as trauma, infection, chronic inflammatory and infectious diseases) cause the progression of primary adrenal insufficiency. Secondary adrenal insufficiency, compared with the primary, proceeds relatively easily.
Symptoms of adrenal insufficiency

most important indicator of the development of primary chronic adrenal insufficiency doctors believe active pigmentation of the skin and mucous membranes, the intensity of which depends on the duration and severity of the disease. First, pronounced dark spots cover the exposed areas of the body, which are most often under the sun's rays - for example, the skin of the face, neck, hands.A characteristic symptom of this pathology is active pigmentation palmar creases( this note and the patients themselves, as the pigmentation perfectly visible against the background of more light skin), darkening of the skin, to a greater extent in contact with clothes.Skin color varies from an easy shade of sunburn, bronze, smoky, dirty skin to pronounced dark - it's all individually. Pigmentation of the mucous membranes( inner surface of the cheeks, tongue, palate, gums, vagina, rectum) is characterized by staining them in a bluish-black color.
Note: is extremely rare in adrenal insufficiency with mild hyperpigmentation - "white addisonism".It is very difficult to diagnose precisely because of the absence of the main feature.
Quite often, both doctors and patients show against the backdrop of bright pigmentation amelanotic bright spots - vitiligo .They can be different in size - from small to large, have an irregular shape.Such discolored spots indicate the development of autoimmune primary hypocorticism of a chronic nature, since it is for this pathology that vitiligo is a characteristic symptom.
In patients with chronic adrenal insufficiency, the body weight decreases from moderate weight loss( 3-5 kg) to significant hypotrophy( by 15-25 kg).
In addition, there are irritability, signs of depression, weakness, lethargy, until disability, a decrease in sexual desire.There is arterial hypotension( lowering of arterial pressure), fainting states caused by psychological upheavals and stresses.Virtually always develop digestive disorders - nausea, decreased appetite, vomiting, pain in the anatomical location of the stomach, loose stools or constipation, anorexia.
Note: if the patient has already been diagnosed with hypertension, and then the development of adrenal insufficiency has begun, then blood pressure indicators may be within normal limits.
At the biochemical level, violations occur:
- protein metabolism( reduced protein synthesis);
- carbohydrate( reduced fasting glucose and flat sugar curve after glucose load) exchange;
- water-salt( hyponatremia, hyperkalemia) exchange.
Patients have an addiction to eating salty foods.Moreover, it is always pronounced - patients begin to dosalivat absolutely everything, can use pure salt, which can be associated with the increasing loss of sodium salts.
Secondary adrenal insufficiency occurs in the absence of a discoloration of the skin, but non-specific symptoms will be present: general weakness and seizures of hypoglycemia that occur within a few hours after eating.
Possible complications of adrenal insufficiency

The most formidable complication of chronic adrenal insufficiency in the case of non-conductive or abnormal treatment is the adrenal( addisonic) crisis of decompensated chronic adrenal insufficiency with the development of coma. Such a life-threatening condition is characterized by acute and intense weakness( up to the state of prostration), a sharp drop in blood pressure( there may be a loss of consciousness, collapse), indomitable vomiting and a loose stool, during which dehydration of the organism actively progresses, the smell of acetone from the mouth, Clonic convulsions, an even greater pigmentation of the skin.Often, with an addisonic crisis, all the symptoms of heart failure appear.
Acute adrenal insufficiency( addisonic crisis), according to the prevalence of symptoms, can occur in three clinical forms:
- Cardiovascular - signs of impaired circulation predominate: pale skin, acrocyanosis, cold extremities, tachycardia, arterial hypotension, threadlike pulse,Collapse, anuria.
- Gastrointestinal - the clinical picture is identical to the signs of food poisoning or symptoms of an acute abdomen( acute pains in the abdomen of a spastic nature, constant nausea, resulting in indomitable vomiting, loose stool with blood impurities, flatulence).
- Neuropsychic - headaches, symptoms characteristic of meningitis, convulsive syndrome, delirium, inhibition, stupor.
Addisonian crisis is very difficult to cure, often even emergency medical care does not give positive results, which leads to the death of the patient.
Diagnosis of adrenal insufficiency
Diagnosis of adrenal insufficiency begins with an assessment of anamnesis, complaints, physical data, finding out the cause of hypocorticism.
Conduct an ultrasound of the adrenal gland that can give the following results:
- if tuberculosis foci or the presence of calcification are detected in the adrenal glands, this indicates the tubercular origin of the pathology in question;
- the presence of autoantibodies to the adrenal antigen21-hydroxylase, the physician diagnoses autoimmune hypocorticism.

To determine the cause of primary adrenal insufficiency, the doctor prescribes the MRI or CT of the adrenal glands .To establish the true causes of secondary adrenocortical insufficiency, it is advisable to conduct CT and MRI of the brain .
If the diagnosis of adrenal insufficiency has given dubious results, the specialist conducts a stimulation test, the input of which is used by hormones produced by the pituitary gland and hypothalamus.This will determine the level of cortisol in the blood - an increase in the level of cortisol by less than 550 nmol / l( 20 μg / dL) indicates adrenal insufficiency.
A general blood test is mandatory, which allows to identify hyponatremia, hyperkalemia, lymphocytosis, eosinophilia and leukopenia - evidence of the development of the primary form of the disease in question.
Treatment of adrenal insufficiency
Modern endocrinology can offer patients with this pathology several methods of effective treatment. The choice of method of treatment depends, first of all, on the cause or provoking factors that led to the development of adrenal insufficiency, and has two goals: elimination of the cause of adrenal insufficiency and replacement of the hormonal deficiency.
Elimination of the cause of adrenal insufficiency implies full-fledged treatment of tuberculosis drugs, diseases of fungal etiology , syphilis;Radiotherapy on the hypothalamus and pituitary gland with the purpose of getting rid of tumors;Operative removal of tumors, aneurysm .In general, the treatment is directed against the underlying disease.But even if the therapy was performed correctly, irreversible processes in the adrenal glands can develop - in this case, the pathology persists, but the patient's condition can be adjusted by lifelong hormone replacement therapy.
Treatment of primary adrenal insufficiency is carried out with preparations of the glucocorticoid and mineralocorticoid series. If hypocorticism occurs in mild form, the physician prescribes cortisone or cortef, in the case of severe pathology, therapy involves prescribing prednisolone in various combinations, cortisone acetate or cortef with mineralocorticoids( deoxycorticosterone trimethyl acetate, DOXA-deoxycorticosterone acetate).
The effectiveness of therapy should be evaluated with regularity, which will allow timely replacement of medicines or adjust dosages.Positive dynamics will be manifested by improved indices of blood pressure, gradual regression of active pigmentation, normal / gradual increase in body weight, improvement in well-being, disappearance of digestive system disorders, anorexia, muscle weakness and stabilization / normalization of the patient's general condition.
There are some more features of treatment of adrenal insufficiency :
- Doses of corticosteroids can be increased 3-5 times if in parallel with the pathology in question the patient has stress factors.During pregnancy, such an increase in the dose of drugs is allowed only in the second trimester.
- Anabolic steroids( nerabolil, retabolil) for chronic adrenal insufficiency are prescribed to patients of different sexes, this therapy is conducted 3 times a year in short courses.
- Diagnosed hypocorticism implies adherence to an individually developed diet, nutrition should be enriched with protein, carbohydrates, fats, sodium salts, vitamins B and C, but with the restriction of potassium salts.
To stop the addisonic crisis:
- rehydration therapy with isotonic sodium chloride solution - daily up to 2 liters of this solution, together with 20% glucose, is administered to the patient;
- intravenous replacement therapy with hydrocortisone or prednisolone, which implies no abrupt withdrawal, but a smooth reduction in the dose of these drugs;
- treatment of pathologies, which served as a provocative factor in the development of decompensated under consideration( more often, antibiotic therapy for infections is required).
Prognosis for adrenal insufficiency
If the diagnosis of the appointment / administration of hormone replacement therapy has been made in a timely manner, then the course of the pathology in question will be favorable.
A single-valued prognosis for adrenal insufficiency will not be given by any specialist, as this depends on carrying out measures to prevent adrenal crises.Moreover, similar measures should be carried out taking into account the acquired infections of injuries and somatic diseases - patients will need to increase the dose of the hormone taken.
Adrenal insufficiency is considered quite a dangerous disease, which, if ignored, can lead to death.Conversely, if the patient strictly observes the appointment of the attending physician, regularly undergoes preventive examinations, predictions will be more than favorable.
Konev Alexander, the therapist


