Craniocerebral injury: symptoms, classification, first aid

The brain is protected from external( mechanical) factors better than any other organ.In addition to the bones of the skull, it is protected from damage to the meninges.The brain-washing fluid also functions as a shock absorber.Nevertheless, craniocerebral trauma( TBI) is one of the most frequent reasons for seeking help in medical institutions.In the general structure of injuries, the share of TBI accounts for more than 50% of cases, and in recent years, there has been a tendency to increase their number, as well as to weight the injuries themselves.Not least this is due to the increase in the pace of life( especially in cities) and the increase in the number of vehicles on the roads. Treatment of craniocerebral trauma is the task of traumatologists and neurosurgeons.In some cases, patients need the help of neurologists and even psychiatrists.
Contents:Consequences of traumatic brain injury
In the case of a head injury,
- may have a mechanical disruption of the integrity of brain tissue;
- disturbance of cerebrospinal fluid dynamics;
- hemodynamic disorders;
- disorders of neurodynamics;
- formation of scars and adhesions.
With concussions, reactive and compensatory changes develop at the level of synapses, neurons and cells.
Contusions are characterized by the presence of visible foci of damage and bruises.

If a brain injury causes damage to stem structures or the hypothalamic-pituitary system, a specific stress response results from a disruption in the neurotransmitter exchange.
The cerebral circulation system is particularly sensitive to traumatic injuries.With CCT, a spasm or expansion of regional vessels occurs, and the permeability of their walls increases.A direct consequence of vascular disorders are disorders of liquorodynamics.
Against the background of CCT, dismetabolic disorders and hypoxia develop.Severe damage can provoke respiratory and hemodynamic disorders.
The so-called "traumatic illness" includes 3 periods:
- acute;
- in between;
- remote.
Depending on the severity and type of TBI, the duration of the first period is from 2 weeks to 2.5 months .The acute phase is determined by the combination of the damaging factor and the defense reactions.This is the time interval from the onset of the impact of the traumatic factor to the restoration of body functions or death.
In the interim period, lysis and reparation processes in the damaged zones are actively proceeding.At this stage, compensatory and adaptive mechanisms that facilitate the return of impaired functions to normal indicators( or a stable compensation) are included.The duration of the second period can be from 6 months to 1 year.
The final( remote) period is characterized by the completion of degeneration and recovery.In some cases, they continue to coexist.The duration of the phase on the background of clinical recovery is 2-3 years, and with the further development of the process it is very uncertain.
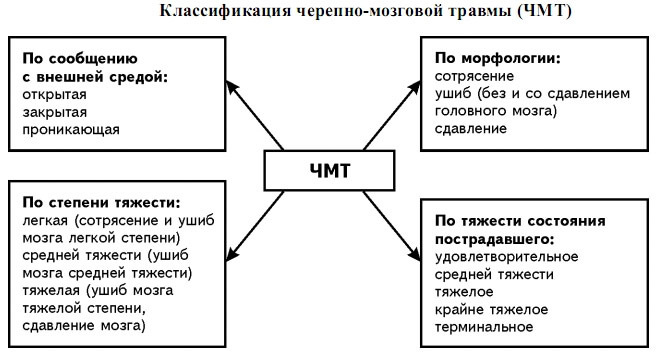
Classification of craniocerebral trauma
Note: injuries of this category are divided into closed, open and penetrating.

Closed CCTs are head injuries accompanied by the development of clinical symptoms, but without serious skin damage.
Open - these are injuries with damage to the layers of the skin and aponeurosis of the skull.
Penetrating injuries are characterized by a violation of the integrity of the hard shell.
Evaluation of the
The following factors must be taken into account in the initial examination and examination of the patient in a medical facility:
-
 condition of the scalp( presence of cuts, crushing and bruising);
condition of the scalp( presence of cuts, crushing and bruising); - presence and localization of fractures;
- the state of spaces under the cerebral membranes( the pressure of the CSF is assessed and subarachnoid hematomas are detected);
- concomitant injuries of various locations;
- the fact of narcotic or alcoholic intoxication( on its background the symptomatology can be smeared).
The severity of craniocerebral trauma is assessed by 3 factors:
- state of consciousness;
- vital functions;
- neurological symptoms.
Gravity grades CCT
- Satisfactory is considered a patient's condition if he has a clear consciousness, there are no violations of the most important functions, there are no primary and secondary neurological clinical signs. With timely and properly conducted therapeutic activities of life, nothing is threatened, and the work capacity is restored to the full.
- For moderate to severe , the mind is clear or there is some stunning.Vital functions do not suffer, but the number of heartbeats can be reduced.Individual focal features can be diagnosed.The threat to life is almost non-existent with the timely provision of qualified assistance. Forecasts for complete recovery after such a traumatic brain injury are quite favorable.
- In severe , the patient is stunned or develops a sopor - depression of consciousness, in which loss of voluntary activity occurs and the reflex is retained.Disturbances of respiratory and circulatory functions are fixed, and neurological symptoms are present.Possible paresis, paralysis and convulsions.The threat to life is quite obvious, and the degree of danger is determined by the duration of the acute phase. The prospects for a complete recovery from severe head injury are questionable.
- Signs of of a very serious condition of are coma, oppression of a number of important functions and pronounced neurological symptoms( both primary and secondary). Threat to life is very serious, and complete recovery from trauma usually does not occur.
- The most dangerous condition is terminal .It is characterized by coma, critical impairments of vital functions, as well as deep stem and cerebral infringements. Unfortunately, it is extremely rare to save the victim in this situation.
Symptoms of craniocerebral trauma
Clinical symptoms allow us to draw preliminary conclusions about the nature of the head injury.
Concussion of the brain
Concussion is accompanied by reversible cerebrovascular disorders.
Symptoms:
- short-lived blackout or loss of consciousness( up to several minutes);
- light stunned;
- some difficulties with the orientation in space;
- memory loss after a trauma;
- motor excitation( rare);
- dizziness;
- headaches( cephalalgia);
- nausea;
- vomiting( not always);
- decreased muscular tone;
- Nystagmus( involuntary swings of the eyes).
During the neurological examination, instability in the Romberg pose may be noted.Symptom, as a rule, quickly regresses.Organic signs pass without a trace in the next 3 days, but vegetative disorders last much longer. The patient may complain of a vascular symptomatology - a decrease or increase in blood pressure, tachycardia, cold snap and blue fingertips, as well as ASH97ASD hyperhidrosis.

Contusions( UGM)
Clinically distinguish 3 degrees of UGM - light, medium and heavy.
Signs of a moderate degree of brain injury:
- loss of consciousness( up to 20-40 minutes);
- cephalalgia;
- vomiting;
- amnesia;
- heart palpitations;
- arterial hypertension( may be absent).
Moderate neurological symptoms regress to the end of 2-3 weeks after such a traumatic brain injury.
Note: is a fundamental difference between the injury and concussion - the possibility of fracture of the bones of the arch and the presence of subarachnoid hematomas.
Symptoms of moderate AMM:
-
 is not conscious until several hours;
is not conscious until several hours; - has amnesia;
- cephalgia( characterized by high intensity);
- repeated vomiting;
- increased or decreased heart rate;
- increase in the frequency of respiratory movements while maintaining rhythm;
- hyperthermia( before subfebrile values).
Neurological examination reveals meningeal and stem symptoms.The main organic manifestations come to naught in 2-5 weeks, but some clinical signs of the suffered craniocerebral trauma have a long history.
Symptoms of severe UGM:
- no consciousness until several weeks;
- is life-threatening violations of critical functions;
- motor excitation;
- paralysis;
- hypo- or hypertonic musculature;
- convulsions.
The reverse development of symptoms proceeds slowly, often residual disorders occur, including - from the side of the psyche.
Important: is a sign with 100% probability of a fracture of the base of the skull - this is the discharge of the cerebrospinal fluid from the ear or nose.
The appearance of symmetrical bruises around the eyes( "glasses"), gives reason to suspect a fracture in the zone of the anterior cranial fossa.
Compression
Compression often accompanies bruises.The most frequent causes of it are hematomas of different localization and damage to the bones of the arch with their impression.Less often, damage is caused by swelling of the brain tissue and pneumo-cephaly.
Symptomatic compression may increase dramatically immediately after a traumatic brain injury or after a certain( "light") time interval.
Characteristic signs of compression:
- progressive impairment of consciousness;
- cerebral disorders;
- focal and stem features.
Probable complications of TBT
The most dangerous in the acute phase are violations of the respiratory system( respiratory depression and gas exchange disorder), as well as problems with central and regional( cerebral) blood circulation.
Hemorrhagic complications are cerebral infarctions and intracranial hemorrhages.
In severe craniocerebral trauma, dislocation( displacement) of the brain is possible.
Against the background of CCT, the probability of complications of a purulent-inflammatory nature is quite high.They are divided into intra- and extracranial.The first group includes abscesses, meningitis and encephalitis, and to the second, for example, pneumonia.
Note: to the number of possible complications include posttraumatic neuroses and epilepsy.
First aid for craniocerebral trauma
 Important: pre-emergency care for head injury is to provide the victim with complete peace of mind.He needs to be given a horizontal position with a raised head.If the patient is unconscious - you can not move it, because you can not rule out the possibility of trauma to the spine.To the head, it is advisable to attach a hot-water bottle with cold water or a packet of ice.If you stop breathing or cardiac activity before the arrival of "ambulance" you need to carry out reanimation measures - indirect cardiac massage and artificial respiration.
Important: pre-emergency care for head injury is to provide the victim with complete peace of mind.He needs to be given a horizontal position with a raised head.If the patient is unconscious - you can not move it, because you can not rule out the possibility of trauma to the spine.To the head, it is advisable to attach a hot-water bottle with cold water or a packet of ice.If you stop breathing or cardiac activity before the arrival of "ambulance" you need to carry out reanimation measures - indirect cardiac massage and artificial respiration.
Primary care for patients is provided at the nearest medical facility.The amount of primary care is determined by the severity of the patient's condition and the capabilities of the physicians. The primary task of physicians is to maintain respiratory and circulatory functions.It is extremely important to restore airway patency( it is often broken as a result of aspiration of blood, secretion or vomit).
All craniocerebral injuries are treated in a stationary . Depending on the nature and severity of the damage, they resort to conservative tactics or perform neurosurgical intervention.
With psychomotor agitation or convulsions in / in the injected relaxants( eg - Diazepam).Symptoms of compression are a good reason for prescribing diuretics.If there is a threat of edema - osmodiuretics are used, and the victim is immediately delivered to the neurosurgical department.
 For the stabilization of blood circulation, vasoactive pharmacological agents are administered, and when probabilities of hemorrhage into the subarachnoid space, hemostatics are indicated.
For the stabilization of blood circulation, vasoactive pharmacological agents are administered, and when probabilities of hemorrhage into the subarachnoid space, hemostatics are indicated.
During the treatment of craniocerebral trauma, neuroprotectors, neuro-metabolic stimulants, vitamin preparations and glutamic acid are widely used.Dehydration medications are needed to combat disorders of liquorodynamics.
The duration of treatment depends on the type and severity of the CCT and the dynamics of the recovery process.Even with light concussions, the patient is shown staying on bed for a week and a half.
Vladimir Plisov, medical reviewer