Tumors of the adrenal glands: symptoms, diagnosis, treatment( removal)

Adrenal tumors are focal neoplasms formed by the growth of cells of the inner( medullary) or outer( cortical) layers.They can have both benign and malignant nature.
Table of contents:Characteristics and classification
The morphological and histological structure of adrenal tumors is variable, as is their accompanying symptomatology.
Among the most common clinical manifestations are adrenal crises.
During the crisis, the patient is noted:
- increased blood pressure;
- heart palpitations;
- pain syndrome( in the chest and abdominal area);
- tremor;
- psychomotor agitation;
- appearance of a sense of fear of death;
- polyuria( increase in the volume of urine leakage).
Note: neoplasms in the adrenal glands often cause metabolic disorders.Against their background, the development of diabetes mellitus is not ruled out.Patients often suffer from sexual function and impaired renal function.
The adrenal glands are one of the most important organs of the endocrine system.
The following hormones are secreted in the cortex:
- androsteroids( androgens, estrogens and progesterone);
- glucocorticoids;
- mineralocorticoids.
Neurotransmitters are synthesized in the medulla:
- epinephrine;
- noradrenaline;
- dopamine.
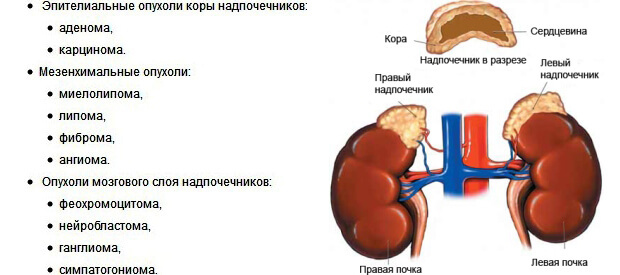
The neoplasm of the adrenal cortex includes:
- corticosteroma;
- corticoestroma;
- aldosterome;
- androsteroma;
- mixed tumors( corticoandrosteromas).
Note: pathological growth of cortical cells is relatively rare.
Internal layer tumors:
- pheochromocytoma( derived from chromaffin tissue);
- ganglioneuroma( proliferation of cells of the nervous tissue).Benign tumors are characterized by a lack of severe symptoms and small dimensions.
Most often, they are accidentally detected during a general examination for other diseases.
Malignant neoplasms tend to rapidly proliferate, and are accompanied by signs of general intoxication. They are divided into primary( derived from adrenal tissue) and secondary( formed from metastases).
Hormonal-inactive tumors
Primary tumors may be hormonally inactive, i.e., not producing any hormones.As a rule, they are benign. Such tumors include fibroids, fibromas and lipomas, often associated with hypertension, metabolic disorders( obesity) and endocrine diseases( diabetes mellitus).Malignant hormone-inactive tumors are very rarely diagnosed.
Hormone-active tumors
 The clinical symptomatology for various types of hormone-secretory tumors depends on which particular biologically active substance begins to be produced in excessive amounts.
The clinical symptomatology for various types of hormone-secretory tumors depends on which particular biologically active substance begins to be produced in excessive amounts.
Aldosteromes grow from the glomerular zone of the cortex, and in excess produce aldosterone.Primary aldosteronism causes a disturbance of water-electrolyte metabolism, increased blood pressure, muscle weakness, hypokalemia and alkalosis. Aldosteromes are more often solitary;Multiple hormone secretion tumors of this type are diagnosed in no more than 15% of cases.In 2-4% of patients, a malignant character is detected by the aldoster.
Corticosteromas( glucosters) are the most common neoplasms of the adrenal glands.They are formed when the cells of the bundle zone of the outer layer grow, they provoke metabolic disorders and hypercorticism. Benign corticosteroids( glucosteromas) are diagnosed more often than malignant( corticoblastomas and adenocarcinomas).
Androsteromas are most often diagnosed in women of childbearing age( 20-40 years). Hypersecretion of sex hormones leads to the appearance of symptoms of masculinization.These tumors( they account for no more than 3% of adrenal neoplasms) can be formed from the mesh cortical layer or so-called.Ectopic adrenal tissue.Against the background of an excess of androgens, early puberty occurs in boys, and pseudohermaphroditism is diagnosed in girls.Women often have symptomatic virilism. Up to 50% androster is malignant.Secondary foci are found in the liver, lungs and lymph nodes of the retroperitoneal space.
Corticoestromes , growing from the reticular and fascicles, lead to estrogen-genital syndrome, which is accompanied by feminization in men.Such tumors are quite rare, but are mostly malignant and characterized by rapid invasive growth.
Pheochromocytomas , secreting catecholamines, in 90% benign ;Malignant course is observed mainly with extra-adrenal localization.These neoplasms appear when the chromaffin cells of the brain layer grow or come from neuroendocrine structures( in particular, the solar plexus).Approximately in every tenth patient with pheochromocytoma, hereditary predisposition is revealed.In women, education data are diagnosed more often.
Symptoms of an adrenal tumor
The asymptomatic course of adrenal tumors is quite rare - no more than 10% of cases.
Aldosteroma
In aldosterome, 3 groups of symptoms develop:
- renal;
- cardiovascular;
- neuromuscular.
Kidney symptoms:
- allocation of the greater part of the daily volume of urine at night;
- strong thirst;
- polyuria;
- urine alkalinization.
These symptoms develop against a background of pronounced hyperkalemia.
Cardiovascular clinical signs:
- resistant to antihypertensives; increased blood pressure;
- shortness of breath;
- intense headaches;
- hypertrophic( later - dystrophic) changes in the heart muscle;
- arrhythmia;
- changes the fundus against the background of persistent hypertension( edema of the optic nerve, retinopathy, hemorrhage).
The crisis that develops against the background of a sharp increase in aldosterone levels is manifested by pronounced myopathy, visual impairment, vomiting and cephalalgia.There are also tetanus and flaccid paralysis.With a crisis, the development of a stroke is possible.
Neuromuscular symptoms:
- Sensitivity disorders;
- muscle weakness;
- convulsions.
Symptomatology is caused by intracellular acidosis and a decrease in the level of potassium in the blood.
Corticosteroma
When forming a corticosteris, the Itzenko-Cushing syndrome develops.
Symptoms of hypercortisone:
-
 central cushingoid obesity;
central cushingoid obesity; - arterial hypertension;
- musculoskeletal weakness;
- increased physical and mental fatigue;
- a violation of the metabolism of carbohydrates( steroid diabetes is not excluded);
- crimson striae( stretch marks) on the skin of the abdomen and thighs;
- point hemorrhages( petechiae);
- osteoporosis( its possible consequence is compression fractures of the vertebrae);
- signs of virilization( in women);
- decreased sexual desire and potency( in men);
- depression;
- is a psychomotor agitation.
Note: in 25% of corticosteroma provokes the development of inflammation of the renal pelvis and stones( stones) in the kidneys.
Corticoesteroma
In girls, corticosteroids lead to an acceleration of sexual and physical development, and in boys - to a slowdown.
Adult men develop feminization symptoms:
- high voice timbre;
- testicular atrophy;
- reduction of the phallus;
- bilateral enlargement of the mammary glands;
- stopping the growth of the beard and mustache;
- reduction or cessation of spermatogenesis;
- lack of potency.
In women, corticostero is manifested only by a high level of estrogens in the plasma.
Androsteroma
The synthesis of androgenes with increased amounts of androgen causes early physical and sexual development in children.In women, virilization is observed, characterized by haemorrhage in the male type, amenorrhea, decreased voice of the voice, uterine hypotrophy, clitoral growth and increased sexual desire.In men, the signs of virilization are more difficult to notice, therefore, androsteromas are usually found in them quite by accident.
Note: sometimes produces androsteromas and glucocorticoids.In such cases, the characteristic symptomatology of hypercortisy develops.
Pheochromocytoma
Pheochromocytoma often causes serious hemodynamic disorders.
There are 3 forms of flow:
- paroxysmal( about 80% of cases);
- constant;
- mixed.
Paroxysmology clinic:
- sharp increase in blood pressure( figures of systolic pressure ≥ 300 mm Hg);
- intense headache;
- hyperhidrosis( sweating);
- pain behind the sternum;
- pallor or "marble" skin pattern;
- tremor;
- nausea and vomiting;
- panic attacks;
- feeling of fear of death;
- increase in the volume of urinary diversion;
- hyperthermia.
Important: can provoke an attack by overeating, drinking, physical work and psychoemotional stress.
The duration of the crisis is up to 2-3 hours, and the frequency of paroxysms is from several times a day to single crises in a few months. The attack is stopped spontaneously - just as suddenly as it begins.Pale skin is replaced by hyperemia.The patient is noted for heavy sweat and hypersalivation.
For , the permanent form of is characterized by persistent hypertension.
With the of a mixed variety of , the flow of pheochromocytoma exhibits both persistent increases in blood pressure and periodic paroxysms.
The severe course of may be complicated by catecholamine shock.It is more common in children.With this condition, hemodynamics becomes uncontrollable, and blood pressure indices change randomly.
Important: The most serious complication of adrenal tumors is their malignancy, followed by the appearance of secondary foci( metastases) in neighboring and distant organs and tissues.Regional lymph nodes are often affected.
Diagnostics
 Currently, diagnostic techniques have been developed that allow not only to detect adrenal tumors, but also to clarify its nature and location.
Currently, diagnostic techniques have been developed that allow not only to detect adrenal tumors, but also to clarify its nature and location.
The degree of activity of hormone-producing neoplasms is determined by the level of hormones, as well as vanillylmandal and homovanilic acid in urine( the whole daily volume is examined).
If the endocrinologist has reason to suspect that the patient has a pheochromocytoma, blood and urine samples are taken during the crisis or immediately after it is completed.This allows us to objectively assess the content of catecholamines.
 A selective phlebography is a very informative tool for studying the hormonal activity of a neoplasm.
A selective phlebography is a very informative tool for studying the hormonal activity of a neoplasm.
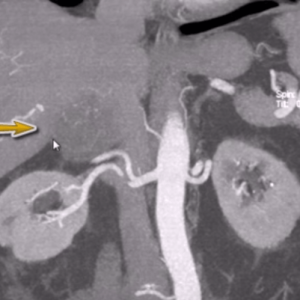
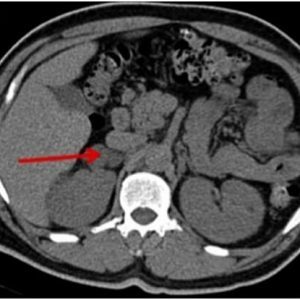
The diameter and precise localization of the neoplasm, as well as the presence of secondary foci, are detected during ultrasound scanning or examination using a tomograph.A hardware examination makes it possible to detect even a hormoneally inactive tumor, the size of which does not exceed 0.5 cm.
Adrenal tumors: treatment and prognosis
Certain types of adrenal neoplasm are treated with the help of Mitotan chemotherapy.
Pheochromocytoma therapy is successfully performed by iv injection of the radioactive isotope a.To combat paroxysms, infusions of nitroprusside sodium, phentolamine and nitroglycerin are practiced.If the conservative measures are ineffective, an emergency operation is indicated.
Unconditional indications for surgery:
- diameter & gt;3 cm;
- hormonal activity;
- signs of malignancy.
 The operation involves removal of the tumor itself and the entire affected organ( adrenalectomy ).When malignant resection is subject to regional lymph nodes.Removal is carried out by open access( through the incision) or using a laparoscopic technique.In the postoperative period, hormone replacement therapy is indicated.
The operation involves removal of the tumor itself and the entire affected organ( adrenalectomy ).When malignant resection is subject to regional lymph nodes.Removal is carried out by open access( through the incision) or using a laparoscopic technique.In the postoperative period, hormone replacement therapy is indicated.
After resection of malignant neoplasms, radiotherapy is additionally performed.
With early diagnosis and timely operation, the prognosis for life is favorable, if it is a benign tumor.
Plisov Vladimir, medical reviewer